-
Cosmedocs| Non Surgical
-
COSMESURG| Surgical
-
HARLEY STREET| Skin Care
FORMULATIONS -
| Skin Bar Clinic
 GLOW & GO
GLOW & GO

10 botox mistakes you should avoid when injecting Botulinum toxin
Undoubtedly, Botox or botulinum toxin holds the title of most demanded non-surgical cosmetic procedure in the world. During the recent years, its use has been combined with dermal fillers which have become a mainstay anti-ageing treatment for preventing and treating signs of facial ageing[1].
Patients who seek injectable treatments generally want to achieve natural results that are minimally noticeable. However, there is a group of people who think that these treatments give un-natural and even grotesque results. There can be two reasons for this thought:
- In few cases, the outcomes of the technique are too paralysing which leads to expressionless face.
- In other cases, the unnatural shape of the eyebrow and other tell-tale lines and wrinkles indicate that a patient has undergone a Botulinum toxin treatment.
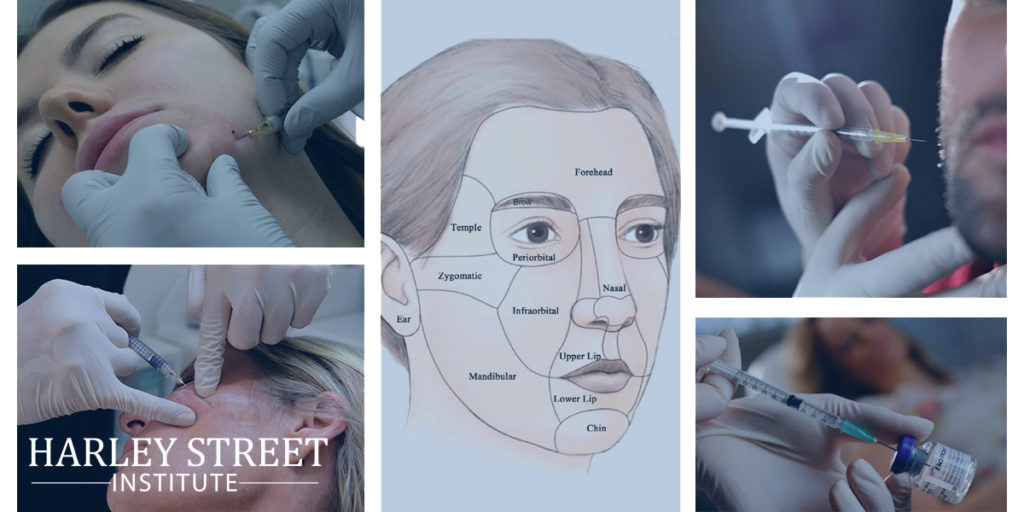
The administration of Botox treatment depends, for the most part, on the understanding and skill of the practitioner. A physician, who has a good knowledge of facial anatomy, as well as the functionality of facial muscles, can deliver outstanding results of the Botulinum toxin treatment. As doctors attending Botox training courses do have an understanding of facial anatomy and muscles, it is a responsibility of the training institute to help them to blend that knowledge with the right injection techniques to deliver natural and enticing results.
It is important to understand that the injection point is not always the problem area for inexperienced injectors. Many Botox horror stories are the result of improper placement, which leads to Botox gone wrong. It is important that a practitioner understands Botox Danger Zones and facial muscles in order to know where to inject Botox.
In this article, we will explore the mistakes which Botox injectors should avoid to achieve excellent results from botulinum toxin treatment.
Five action errors
- Using excessively high dose of botulinum toxin
The use of high Botox dose usually results in loss of expressions. In some articles and textbooks, the recommended dose of botulinum toxin type A injections is 20-40 Units for the glabella region, 15-30 units for the forehead and 12-30 units for the crow’s feet[2]. But this recommended dose may give un-natural results so we curtail this dosage depending on individual client. For the glabella 30% less, for forehead 50% less dose is used while dose for crow’s feet remains same to give natural looking results. For the lower face, usually 50% less than the recommended dose produces natural results with fewer side effects.
However, it is important to inform patients that the effects of this approach will last for a shorter period (approx. 3-4 months). With this protocol, ask the patient to return for follow-up treatment two weeks following the initial treatment. The practitioner, then, reassesses the patient and makes adjustments. If required, practitioner injects an additional dose of Botulinum toxin injections in some facial areas. Help your patient, to understand that less is more in the case of botox.
- Injecting the Frontalis Muscle Instead of the Corrugator Supercilii Muscle
This action results in creating a Mephisto effect. In most of the textbooks as well as botox training courses show five traditional injection sites of the glabellar region. But practically speaking, the 2 of these superior injection sites are not actually located in the corrugator supercilii muscle, which makes the insertion site nearly at the eyebrow level.
The injection sites are located actually on the frontalis muscle so that the relaxation of this muscle makes the medial eyebrow portion to descend while lifting the lateral brow portion which results from compensatory lateral fibres contraction of the frontalis muscle. This action results in a Mephisto effect or devil brow.
In some cases, a higher concentration of botulinum toxin is used to achieve greater precision and to relax just the corrugator supercilii muscle. With this approach, lesser volume of liquid is injected which decreases the likelihood of diffusion to untargeted muscles (in this instance, the frontalis).
- Always Injecting the Superior-Lateral Portion of the Orbicularis Oculi Muscle
This action results in the excessively elevated eyebrows. Botulinum toxin infiltration through the superior-lateral fibres of the orbicularis oculi muscle helps to relax those fibres and also lifts the lateral brow portion. The problem is that the eyebrow position in some patients moves upward with ageing due to physiological contractions of the frontalis muscle.
It was found in one of the study[3] that physiological eyebrows elevation tends to occur with ageing in most of the patients. Therefore, to achieve natural results, superior-lateral fibres of the orbicularis oculi muscle should be injected in case the lateral portion of the brow has dropped among patients.
- Injecting the Frontalis Muscle in Patients Who Use it to Raise the Eyelids
This action leads to brow or eyelids ptosis. It has been observed in many patients over the age of 65 years or above that they use frontalis muscle for keeping their eyes open. The relaxation of frontalis muscle in such patients can result in brow or eyelids ptosis. Therefore, while injecting botulinum toxin injections in these patients, the doctor should carefully examine that whether the patient use frontalis muscle for opening eyes or not. If yes, the injection should be avoided in that.
- Injecting too low in the crow’s feet
This results in undereye bags exacerbation. Some patients have under eye bags due to herniated fat or retention of fluid. In both cases, if orbicularis oculi inferior muscle fibres are excessively relaxed with the injections of botulinum toxin, it further aggravates the appearance of these bags. Therefore, in patients who have a tendency of developing under eye bags, the most inferior portion of crow’s feet should not be injected to maintain the tone of collateral orbicularis oculi muscle region.
Five Omission errors
- Failure to inject lower third portion of the face
This error results in giving less effective overall results. While administering Botulinum toxin injections, the effect of injections on the whole face of the patient should be considered with the objective of main depressor muscle relaxation in upper as well as a lower third of the face. High doses of botulinum toxin in the lower third of the face can lead to cosmetic and functional problems so it is necessary to inject low doses to avoid any complications.
In the lower third portion of the face, the platysma muscle at the jawline (using a technique called the ‘‘Nefertiti lift’’)[4], the depressor septi nasi muscle (in patients with a plunging nasal tip while smiling)[5], the depressor anguli oris muscle (for lifting mouth corners)[6], the mentalis muscle (for relaxing ‘‘pebbly’’ effect caused by the insertion of this muscle on the skin)[7], etc. can be relaxed.
Some patients have hypertrophy of masseter muscle which causes functional (bruxism) as well as cosmetic (square jaw) alterations. The injection of botulinum toxin into this muscle not just improves bruxism symptoms but also changes the square jaw line into a more oval shape[8].
- Failure to inject wrinkles formed due to botulinum toxin
This gives unnatural wrinkles. Due to relaxation of certain muscles with botulinum toxin, the tone of adjacent muscles increases to compensate the inactivity of treated muscles. This action helps in creating a desirable lifting effect but it also causes wrinkles in other areas which should be corrected through botulinum toxin treatment.
- Lack of familiarity with the patterns of muscle contractions
This lack of knowledge gives an unnatural appearance. The approach of ‘one size fits all’ does not work in the case of Botulinum toxin treatment. The suitable sites of injection depend on individual patient’s muscles contraction pattern. Therefore, it is necessary for the practitioners to understand the contraction patterns of glabella, forehead and crow’s feet. This information will enable them to custom tailor the injection pattern for each patient giving more natural results with a smaller quantity of botulinum toxin.
- Failure to distinguish between eyebrows of males and females
This inability can lead to giving masculine appearance to females and feminine appearance to males. The women’s eyebrows have a classic shape of ‘seagull wing’ while the eyebrows of men are straighter and closer to the upper eyelid. By relaxing frontalis muscle eyebrows can be shaped or by relaxing the orbicularis oculi muscle superior-lateral fibres, the lateral portion of the brow can be lifted. The botulinum injections should be injected into three depressor muscles for lifting the medial eyebrow portion including the procerus, the corrugator supercilii, and the depressor supercilii.
- Failure of combining Botulinum toxin with other aesthetic treatments
Botulinum toxin injections offer outstanding results for reducing certain expressions lines and wrinkles however the combination of botulinum toxin with other cosmetic treatments gives excellent overall outcomes and practitioners should explain this to the patients. For instance, along with lines and wrinkles, another clear sign of ageing is a loss of facial volume. This is why dermal fillers and botulinum toxin treatment is often combined to achieve naturally impressive results.
During the botox training courses, these errors should be kept in view and the trainees should be trained to address these errors, competently.
References
[1] Cartee TV, Monheit GD. An overview of botulinum toxins: Past, present, and future. Clin Plast Surg. 2011;38:409—26.
[2] . Alam M, Dover JS, Klein AW, Arndt KA. Botulinum A exotoxin forhyperfunctional facial lines: Where not to inject. Arch Dermatol.2002;138:1180—5.
Stephan S, Wang TD. Botulinum toxin: Clinical techniques,applications, and complications. Facial Plast Surg. 2011;27:529—39.
[3] Matros E, Garcia JA, Yaremchuk MJ. Changes in eyebrow position and shape with aging. Plast Reconstruct Surg. 2009;124: 1296—301.
[4] . Levy PM. The ‘Nefertiti lift’: A new technique for specific re-contouring of the jawline. J Cosmet Laser Ther. 2007;9:249—52.
[5] Redaelli A. Medical rhinoplasty with hyaluronic acid and botulinum toxin A: A very simple and quite effective technique. J Cosmet Dermatol. 2008;7:210—20.
[6] . Choi YJ, Kim JS, Gil YC, Phetudom T, Kim HJ, Tansatit T, et al. Anatomical considerations regarding the location and boundary of the depressor anguli oris muscle with reference to botulinum toxin injection. Plast Reconstruct Surg. 2014;134:917—21.
[7] Beer K, Yohn M, Closter J. A double-blinded, placebo-controlled study of Botox for the treatment of subjects with chin rhytids. J Drugs Dermatol. 2005;4:417—22.
[8] Klein FH, Brenner FM, Sato MS, Robert FM, Helmer KA. Lower facial remodeling with botulinum toxin type A for the treatment of masseter hypertrophy. An Bras Dermatol. 2014;89:878—84.
Wu WT. Botox facial slimming/facial sculpting: The role of botulinum toxin-A in the treatment of hypertrophic masseteric muscle and parotid enlargement to narrow the lower facial width. Facial Plast Surg Clin North Am. 2010;18:133—40.
Related Posts




X
We use cookies to give you the most relevant experience, Cookie Policy.
Start Your Aesthetic Career
Foundation
Botox & Dermal Filler Course
Botox & Dermal Filler Course
£950* (RRP £1190)
*excluding VAT
*excluding VAT
Limited Time Offer
See What Our Fellows Have Been Up to Recently
Understanding depth, volume, and pressure can enhance a practitioner’s skill set, enabling them to provide more valuable services to their clients using their existing tools. #aestheticmedicine #dermalfillertraining #wrinklefree
{kind=link}
Mastering hand stability isn’t magic, it’s a mix of experience & targeted learning 🎯 Our students get ahead with specialized techniques, paving the way for precise injections! 💉#SkillDevelopment #FutureHealthPros
.
.
.
.
.
#dermalfillertraining #aestheticmedicine #botoxtraining
{kind=link}
{kind=link}
Virtually any area can be reached using a cannula #fillertraining #aestheticmedicine #hsifellowprogram
{kind=link}
“Unlock Your Aesthetic Potential with Harley Street Institute’s Fellowship! 🌟 Elevate your skills in aesthetic medicine through our intensive hands-on training in Botox and Dermal Fillers. Get ready to sculpt beauty, one injection at a time! 💉✨ Join us for a transformative learning journey that takes you beyond the classroom and into real-world expertise. Are you ready to master the art of enhancing natural beauty? 💫 #HarleyStreetFellowship #AestheticMedicineMastery #SculptingBeauty”
{kind=link}
Link in bio
"Unlocking the Secrets of Masseter Botox: Empowering smiles, one injection at a time! 💉💪 Join me on an exciting journey as we delve into the world of Masseter Botox. Learn the art and science behind this transformative procedure, and discover how it can redefine facial aesthetics. Don`t miss out on this opportunity to enhance your skills and expand your practice. Let`s reshape faces and build confidence together!
Link in bio.
#MasseterBotoxCourse #FacialAesthetics #TransformativeProcedures #SmileEnhancement #ContinuingEducation
#aestheticmedicine
{kind=link}
💭Have You Ever thought :
👉🏼What lies beneath the orbicularis oculi ?
👉🏼Why do I need to have the correct depth ?
👉🏼How to avoid an asymmetric smile, periorbital edema or a shelf like look at the lid/cheek junction ?
⚠️We all know that when treating crows feet, we are administering botox into the orbicularis oculi, and that there are complications but which and how?
‼️Too inferior or deep🟰 an asymmetric smile
(you’ve hit the zygomaticus minor muscle and major if you’re really too inferior!)
‼️Too medially 🟰 periorbital edema
(and you’re the periorbital region )
Located just underneath the skin, the orbicularis oculi has multiple origin and insertion points. A paired muscle, that overlies the periorbital region in a circular manner.
⚠️The wrong location, the wrong depth can result you injecting botox into a completely different muscle.
{kind=link}
Welcome to the under eye region, an area of the face that can often show signs of aging such as wrinkles, hollows, and dark circles. Today, I want to share with you how fillers can be used to address these concerns by injecting them into different layers of the skin.
Using a needle, we can inject fillers into the dermis layer of the skin to improve the appearance of fine lines and wrinkles. This can help to smooth out the texture of the skin and create a more youthful and refreshed look. However, it’s important to note that injecting fillers into this layer requires specialized training and experience to ensure safe and effective results.
In addition to the dermis layer, fillers can also be injected into the bone to help address deeper hollows and shadows under the eyes. This technique requires a higher level of expertise as it involves precise placement of the filler to achieve the desired outcome.
Lastly, fillers can be injected into the fat compartment of the under eye region using a cannula. This method can help to add volume and smooth out any irregularities in the fat pads under the eyes. Again, specialized training and experience are crucial for safe and effective results.
Overall, the use of fillers in the under eye region can provide a non-surgical solution to address signs of aging and enhance the appearance of the face. However, it’s important to seek out a qualified and experienced provider who has received proper training in the use of fillers in this delicate area.
If you’re interested in learning more about how fillers can benefit you, please don’t hesitate to reach out and schedule a consultation. Let’s work together to help you achieve your aesthetic goals!
#cosmedocs #harleystreetinstitute
.
.
.
.
#lifestyleblogger
#selfcarematters #aestheticmedicine
#beautytips
#skincarecommunity
#antiagingtips
#makeuptutorials
#selfcarelove
#aestheticbeauty
#lifestyleinspo #lifestyleblogger
#selfcarematters #dermalfillertraining
#beautytips
#skincarecommunity
#antiagingtips
#makeuptutorials
#selfcarelove #dermalfillers
#aestheticbeauty
#lifestyleinspo
#antiagingsecrets
#harleystreet #drahmedhaq #oxforduniversity
#harleystreetinstitute
{kind=link}
The mentalis muscle is a facial muscle located in the chin area. It originates from the mandible and extends downward to the skin of the chin. The primary function of the mentalis muscle is to control the movement and position of the lower lip and the skin of the chin. It plays an important role in activities such as speaking, smiling, and pouting.
In addition to its role in facial expression, the mentalis muscle also helps to maintain the position of the lower front teeth and the shape of the lower lip. Dysfunction or hyperactivity of the mentalis muscle can lead to the development of chin wrinkles, which are vertical lines that appear on the skin of the chin. Understanding the anatomy and function of the mentalis muscle is important for healthcare providers when performing aesthetic procedures in the chin area.
Online Course With Video Demo
www.harleystreetinstitute.com
#botoxtraining #mentalistreatment
{kind=link}
#Repost @dranabilamzavala with many thanks 🙏 and best wishes for the future.
Esta semana tuve la oportunidad de estar en Londres en una de las mejores clínicas con los mejores equipos de Medicina Estética en el mundo, perfeccionado técnicas de Rinomodelación con el Dr.Ahmed Haq.
——
@drahmedhaq You are simply incredible, thanks for the hands on and all the new techniques you shared. @drahmedhaq @harleystreetinstitute @cosmedocs
.
.
.
#aestheticmedicine #dermalfillertraining #nosejob #medicaltraining #plab #harleystreet #10harleystreet #aesthetics
{kind=link}
{kind=link}
Huge Congratulations to Mariana, on completing her foundation course in Aesthetics Medicine with us here at Harley Street Institute. 🥇✨
This combined course covers the necessities required for daily clinic practise, whether starting out or refreshing skills. Our small group training (4:1) provide unparalleled mentorship at any of our training days.
#cosmetictraining #aesthetics #hsi #cosmetics #cosmedocs #harleystreetcourses #foundationcourse #london
{kind=link}
{kind=link}
Only courses with true mentorship. #botoxtraining #dermalfillertraining #aestheticmedicine #hsifellowprogram #harleystreetfellowship
{kind=link}
Huge congratulations to @onemedicalclinic for completing her Fellowship in aesthetic Medicine with us at Harley Street Institute 💫💫✨ We are so proud of having you 🥰
#Repost
Dr Crystal:”When I completed medical school 13 years ago, one of my cherished mentors gave me advice that has stayed with me for life - “never stop learning; it makes the difference between being good and being great."
From my years of Ophthalmic-surgical training to becoming a student of Public Health to my experience as a legislator in Parliament to operating my own
Medical and Aesthetic Medical practice, the lessons learned have been varied and valuable. 🤓
On this occasion my commitment to lifelong learning led me to Harley Street, London. I didn’t just want to be a good injector, I needed to be a great one so I needed to go where the great injectors were. 💉
Every day for the last two months I was immersed in one-on-one intensive training with the aim of mastering my injectable skills and thanks to the incredible team of doctors and trainers at @cosmedocs
@harleystreetinstitute l am proud to say Mission Accomplished! “
{kind=link}
Huge Congratulations to Dale Rae for completing the Certificate in Aesthetic Medicine training program. 💫💫
💉The 3-day Aesthetic Medicine Certificate is tailored towards new practitioners who are ready to kick-start their career in Aesthetic Medicine. It aims to provide an in-depth understanding of the Layers of the Skin and Biological Ageing Process. The package also includes our most popular Foundation Botulinum Toxin and Dermal Fillers course, including an introduction to using cannula.
💉It is an Intense 3-day course incorporating essentials basic and advanced botox and dermal filler procedures combined with popular skin treatments perfect for the beginner all-rounded aesthetic practitioner.
You will be provided direct mentorship by our various cosmetic practitioners who are experts in performing their respective aesthetic treatments.
💉Small group training under the direct supervision of our experienced aesthetic trainers. Master procedures to an advanced level. Learn theory, consultation methods and manage client expectations as well as complications.
🙌 DM for more details. #aesthetic #dermalfillers #detmalfillertraining
{kind=link}
Aesthetic medicine is an art. It`s not enough to know facial anatomy or to be a good injector. The best aesthetic doctor has an artistic eye. Sometimes this is a skill that can be developed over years. Being able to assess a fa ce within seconds of walking into a room. Knowing exactly how injectables can be used for subtle and natural results.
The end result should not be obvious to an untrained eye.
It`s such a shame to see overfilled faces exaggerating proportions. When really, the main aims are to restore volume lost or correct natural imbalances.
#aestheticmedicine #dermalfillers #beauty
Repost @cosmedocs
{kind=link}
Huge Congratulations to @erikatydermatology for completing her Fellowship in Aesthetic Medicine with us at the Harley Street Institute 💫💫💫
Our Aesthetic Fellowship is the pinnacle of training for those seriously interested in escalating their careers.
.
Our fellows are taken on board within clinic over 3 months with weekend workshops, 1-1 mentoring, treatment log book and clinical assistance.
.
Following on from this they have the opportunity to have Independent Fellow Clinics to improve their confidence with patient consultation and individual treatment planning.
.
We believe that this is the future of aesthetic traning to ensure that practitioners have captured all the essential skills for successful careers.
.
We have been extremely proud of our old fellows, many who have moved on to now work with some of the most prestigious clinics in London.
.
Next enrolment periods: TBC
.
To find out more information or to apply, please email your CV to [email protected]
.
#thefellowship #harleystreetinstitute #doctorsanddentists
{kind=link}
{kind=link}
KISS
As the years some procedures get unnecessarily more complicated without much added benefits. Risks / complications have increased: more inexperienced practitioners , inadequate techniques, increasing consumer demand for bolder augmentation.
#keepitsimplestupid
{kind=link}





![]()
![]()
X
Thank you!
For Contacting US. Please check your inbox, we have sent you the Download link
Note: if you did not get the email, please check spam/junk folder
Note: if you did not get the email, please check spam/junk folder